Human Health & Real-World Risk
Are microplastics harmful to human health?
Bottom line: No credible evidence currently shows that normal real-world exposure to microplastics harms human health.
Actual doses people encounter in food, water, air, and dust have not been shown to cause any effects in humans. Animal toxicity testing (both short and long-term) shows plastic materials like polyethylene, polypropylene, PET (polyester), PVC and polystyrene to be some of the lowest toxicity materials we encounter. There is not an absence of evidence because we have toxicology studies spanning many decades.
Sources: Plastics Research Council; WHO 2019 and 2022; FDA 2024; Koelmans 2022; SAPEA 2019; Merski 2008; Stock 2021; Styles 1973
What does the evidence actually show?
Bottom line: The evidence shows that very small amounts of plastic particles may be reported in food, water, air, dust, and some biological samples. It does not show that these findings cause disease.
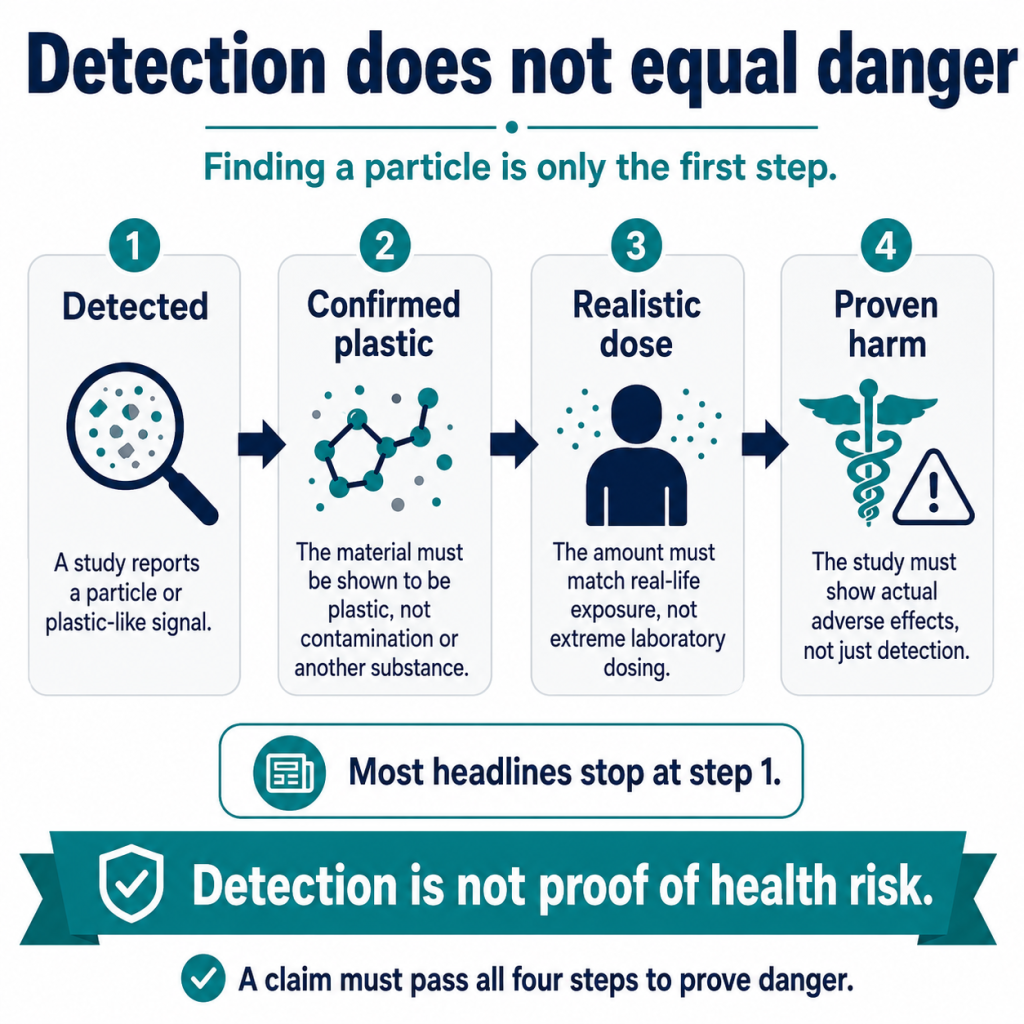
The key distinction is simple: detection is not danger. To show danger, a study must prove the particle identity, measure a realistic dose, show that the particles reach a relevant part of the body, and demonstrate harm. Plastic is a very minor component of dust, which is virtually everywhere, and therefore we find plastic particles wherever dust is found.
Sources: WHO 2019; WHO 2022; EFSA 2016; FDA 2024; Koelmans 2022; SAPEA 2019; Gouin 2022
Are microplastics toxic, or are they mostly inert particles?
Bottom line: Common plastic particles are among the least chemically reactive particles people encounter.
Toxicity depends on dose, size, shape, chemistry, and exposure route. At realistic exposure levels, ordinary plastic particles have not been shown to cause human disease. For example, long-term animal feeding studies report no observed adverse effects even when polymer material made up about 5% or more of the diet (Merski 2008; Styles 1973; Stock 2021). That applies to common plastics like polyethylene, polypropylene, PET (polyester) and uPVC for example. The toxicity is lower than it is for table salt, or caffeine. Plastics are recognized as some of the lowest toxicity substances known. PTFE (known as Teflon®; one member of the PFAS group) was reported to show no toxicity when fed at 25% of the diet for months. In contrast, cement and concrete are used in vastly higher quantities than plastic and there are many studies showing toxicity from that type of dust.
Sources: Merski 2008; Stock 2021; Naftalovich 2016; Wieland 2022; DeArmitt 2025; Nordby 2011; Shansal 2021; Ramani 2018; Cetintepe 2025; Ahmad 2021; Omidianidost 2019; Meo 2013
Do microplastics in the environment prove a human health risk?
Bottom line: No. Environmental detection is not proof of human harm.
A material can be detectable in water, air, soil, sediment, or wildlife without being present at a dose that causes disease in people. OSHA treats low-toxicity dusts without their own chemical-specific standards as particulates not otherwise regulated, historically called nuisance dust (OSHA 2023; OSHA Table Z-1; NIOSH 2026). This is the low-toxicity dust category used when no substance-specific standard applies. Particles not otherwise regulated (PNOR) are associated with inhalation toxicity (not systemic, but physical toxicity). The Permissible Exposure Limit (PEL) is 15 mg/m3 per 8-hr time weight average which is lower than many other PELs (see 29 CFR 1910.1000).
Sources: OSHA 2023; NIOSH 2026; Wieland 2022
Should people be worried about microplastics in the body?
Bottom line: No. Normal microplastic exposure is not a reason to avoid plastics or change everyday behavior.
People are exposed to many particles every day: food particles, mineral dust, soot, textile fibers, skin flakes, pollen, cellulose, and other debris. Plastic appears to be only a small part of total particle exposure. Concern should be proportional to measured dose and proven harm.
Sources: Plastics Research Council; WHO 2022
Do microplastics cause disease?
Bottom line: No human disease has been proved to be caused by normal microplastic exposure.
Some studies report associations or laboratory effects. That is not proof of disease in humans. Many alarming studies use artificial particles or doses far beyond real life, sometimes a million times higher than realistic environmental levels. Those studies do not show that normal exposure makes people sick.
Sources: Lenz 2016; WHO 2022; Koelmans 2022; SAPEA 2019; FDA 2024
What is the difference between finding microplastics and proving harm?
Bottom line: Finding something is not the same as proving it is harmful.
A laboratory may report a plastic-like particle or polymer signal. That only answers the question “what might be present?” It does not answer “is it dangerous?” Harm requires proof of dose, exposure route, persistence, and biological damage at realistic levels. There is no evidence of harm even after extensive testing.
Sources: WHO 2022; FDA 2024; Koelmans 2022; SAPEA 2019; Bradford Hill 1965
How much microplastic are people actually exposed to?
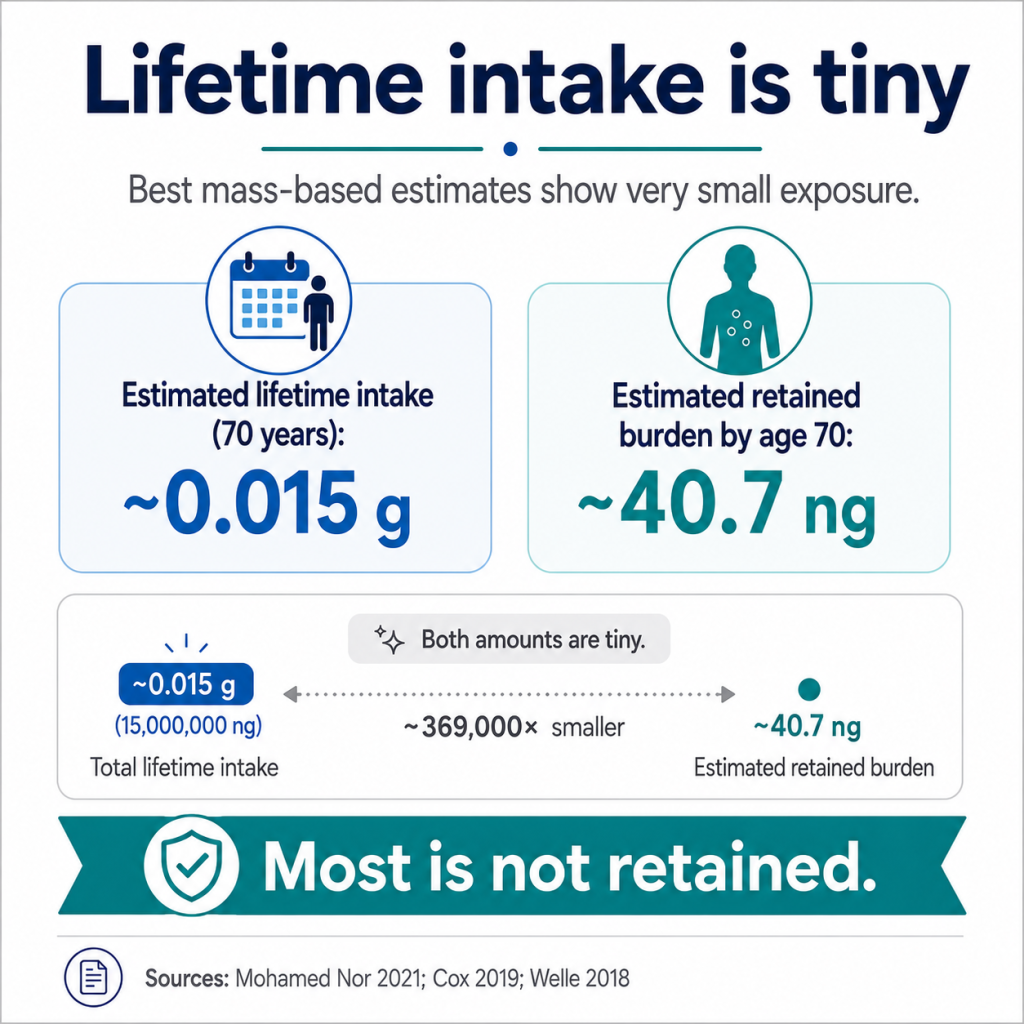
Bottom line: Best mass-based estimates indicate that exposure is very small.
Mohamed Nor et al. estimated median adult intake at about 583 nanograms per day for microplastics in the 1–5000 µm range, or roughly 0.015 g over 70 years before accounting for elimination. The same model estimated adult tissue burden by age 70 at only about 40.7 ng. That means the modeled retained mass is roughly 0.00027% of lifetime intake. These numbers are incompatible with claims that the body contains grams of plastic.
Sources: Nor 2021; Cox 2019; Welle 2018; Senathirajah 2021
How far below no-effect and occupational benchmark levels is normal microplastic exposure?
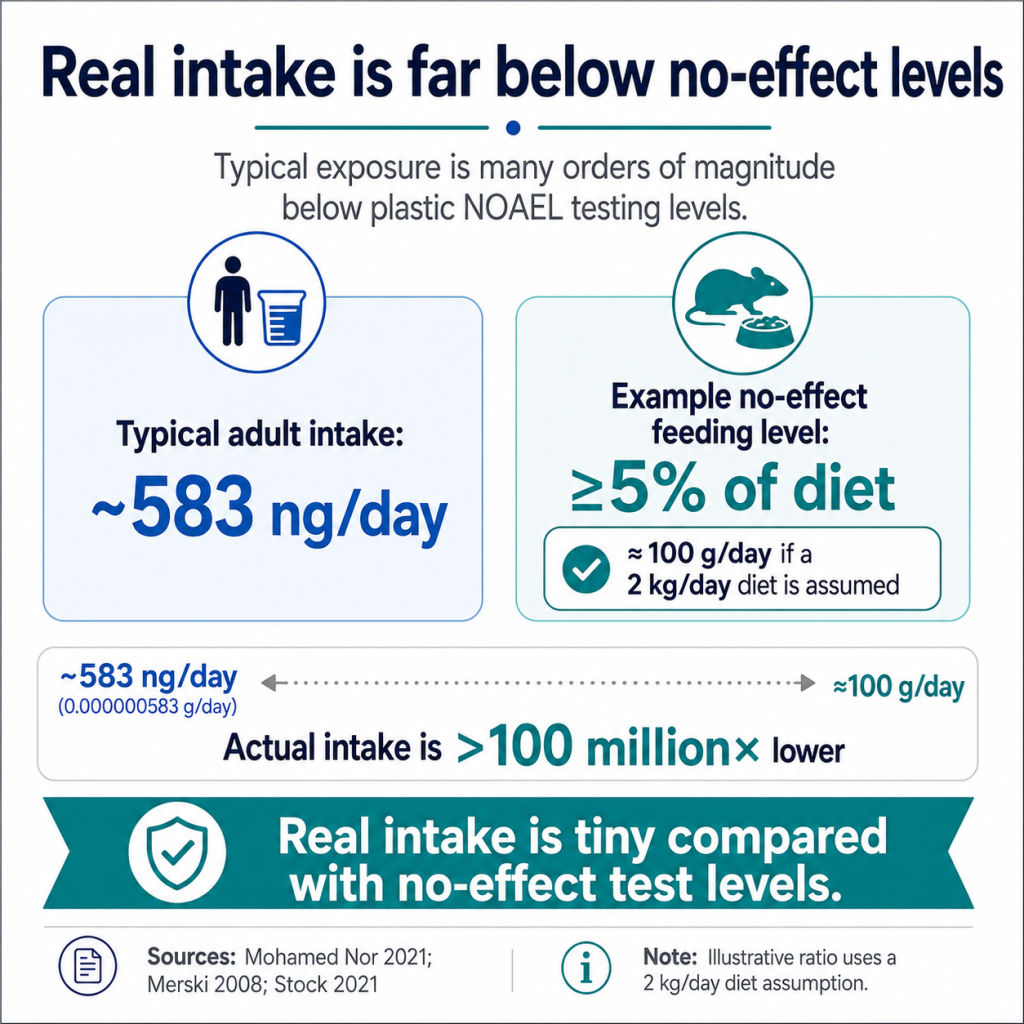
Bottom line: Normal exposure is not close to harmful-dose levels. For ingestion and inhalation, measured or modeled exposure is thousands, millions, or even more times lower than established no-effect or workplace dust limits.
For ingestion, Mohamed Nor et al. estimated median adult intake at about 583 nanograms per day, or 0.000000583 grams per day (Mohamed Nor 2021). In long-term animal feeding studies, common plastics such as polyethylene and PET have shown no observed adverse effects even when polymer material made up about 5% of the diet (Merski 2008; Styles 1973; Stock 2021). For an adult eating roughly 1-2 kg of food per day, 5% of the diet is about 50-100 grams per day. Compared with 0.000000583 grams per day, normal estimated intake is roughly 80 million to 170 million times lower than that 5%-diet no-effect benchmark.
Even if a microplastic exposure estimate were wrong by a factor of 1,000, the exposure would still be tens of thousands to hundreds of thousands of times below that kind of no-effect dietary level. That is the point the public rarely hears: the actual mass swallowed is tiny compared with doses shown not to cause harm.
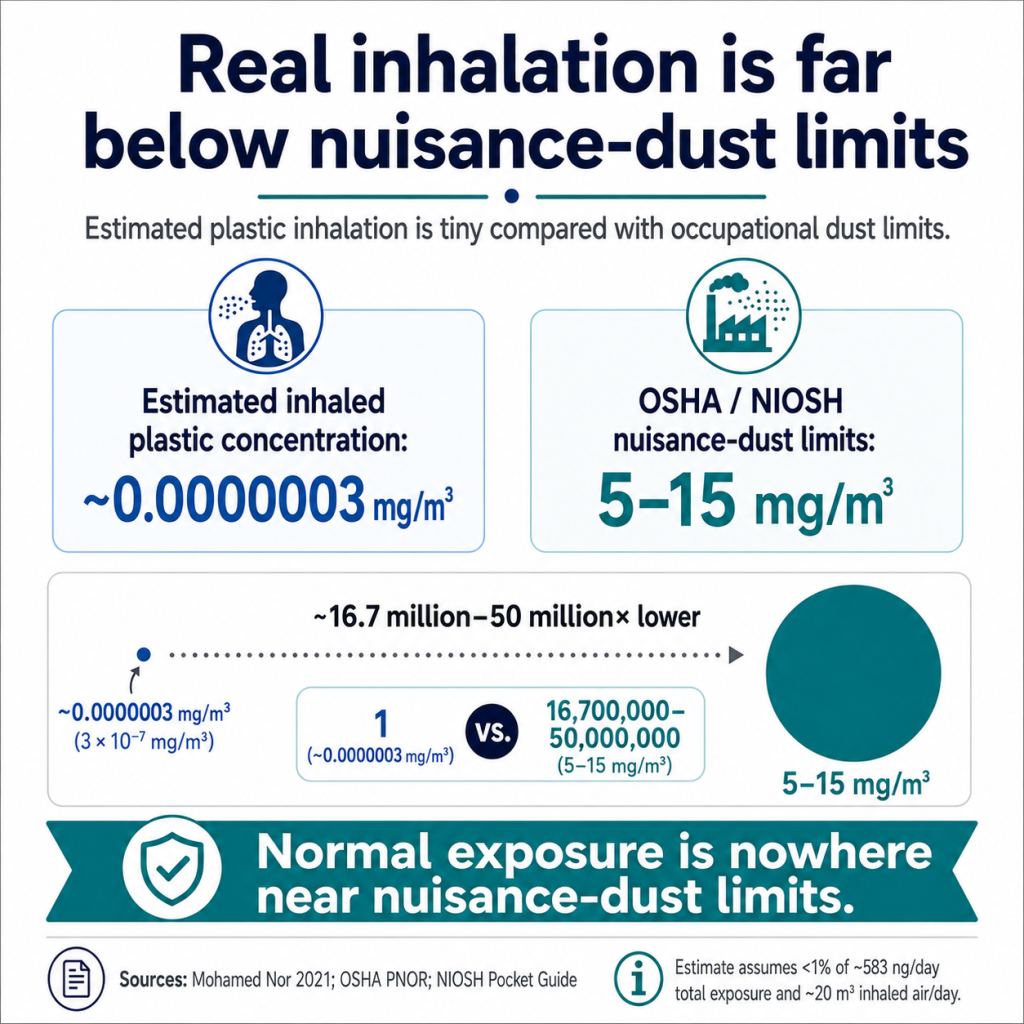
For inhalation, the same dose reality applies. OSHA treats low-toxicity dusts without a specific standard as particulates not otherwise regulated, historically called nuisance dust (OSHA 2023; OSHA Table Z-1). The OSHA permissible exposure limit is 15 mg/m3 for total dust and 5 mg/m3 for the respirable fraction as an 8-hour workplace average (OSHA 2023; OSHA Table Z-1; NIOSH 2026). Those limits apply to total low-toxicity dust, not just plastic dust. Normal environmental inhalation of plastic particles is far below those workplace dust levels because plastic is only a small fraction of airborne dust and the modeled plastic mass inhaled is extremely small. For comparison, EPA assumes workers breathe 10 m3 air/8-hr day so at the respirable PNOR PEL, worker exposure is 50 mg/work day.
Using the respirable-dust limit alone, 5 mg/m3 over a typical workday can correspond to tens of milligrams of low-toxicity dust inhaled during the day (OSHA 2023; OSHA Table Z-1). Modeled microplastic inhalation is in the nanogram-per-day range (Mohamed Nor 2021; Eberhard 2024). That puts normal inhaled plastic exposure millions of times below the OSHA respirable nuisance-dust level. Again, even large uncertainty in the estimate would not bring normal exposure close to the occupational limit.
This does not mean people should deliberately breathe dust or eat plastic. It means that risk has to be proportional to dose. When actual exposure is millions of times below levels that produce no observed harm or below workplace limits for low-toxicity dust, claims of a normal-exposure health crisis need extremely strong evidence. Current evidence does not provide that.
Sources: Nor 2021; Mohamed Nor 2021; Merski 2008; Stock 2021; OSHA 2023; NIOSH 2026; Wieland 2022
How do real-world exposures compare with doses used in toxicology studies?
Bottom line: Many laboratory studies use doses far above real life.
Many laboratory studies use doses hundreds, thousands, or millions of times higher than real life. That is not a small technical detail. It changes the meaning of the result. At extreme doses, even ordinary dust or soil particles can cause reactions. Lenz showed that many studies use plastic-particle concentrations a million times or more above real environmental levels (Lenz 2016). Those studies do not prove that everyday exposure is harmful.
Sources: Lenz 2016; Eberhard 2024; Burns 2018
Why do many harm studies fail to represent real-world microplastics?
Bottom line: They often use the wrong dose, the wrong particles, or the wrong exposure conditions.
Common problems include unrealistically high concentrations, perfect spherical polystyrene beads that do not represent normal exposure, weak controls, poor contamination prevention, and results that are never compared with real human dose. These are not minor weaknesses. They can turn an artificial laboratory result into a frightening headline that does not apply to real life.
Sources: Lenz 2016; Gouin 2022, Eberhard 2024, Koelmans 2019; Cowger 2020; Hermsen 2018
Why did some early microplastics harm studies mislead the public?
Bottom line: Several early high-profile microplastics harm studies raised alarms before the field had strong agreement on realistic dose, representative particles, contamination control, or appropriate controls.
Early microplastics studies attracted wide public attention because they appeared to show dramatic harm to fish, oysters, and other aquatic organisms. Those studies were important in bringing attention to particle pollution, but many were later criticized because they did not represent normal environmental exposure. Common weaknesses included extreme particle concentrations, artificial laboratory polystyrene beads, nanoparticles rather than the larger particles most often measured in the environment, chemically pre-loaded particles, weak comparison particles, missing or limited dose-response data, and conclusions that were treated as broader than the experiment justified.
Examples illustrate the problem. Wardrop et al. reported transfer of sorbed pollutants from ingested microbeads to fish; that result depended on chemically contaminated microbeads and should not be read as proof that normal microplastic exposure is an important chemical-delivery pathway. Sussarellu et al. reported reproductive effects in oysters exposed to polystyrene microplastics, but the relevance of the tested particles and concentrations to normal environmental exposure was later questioned. Barboza et al. reported increased mercury bioconcentration and oxidative stress in European seabass exposed to microplastics and mercury, but that is a combined chemical-plus-particle exposure scenario, not evidence that ordinary plastic particles alone cause harm at realistic concentrations. Lu et al. reported uptake and liver effects in zebrafish exposed to polystyrene microplastics and nanoplastics, but the study used laboratory polystyrene particles and was later specifically criticized for uncertainty about particle identity and interpretation. Mattsson et al. reported behavioral and metabolic effects in fish exposed to polystyrene nanoparticles, but nanoparticle experiments should not be generalized to ordinary mixed environmental microplastics without realistic exposure comparison.
The most serious example was the high-profile Lönnstedt and Eklöv larval-fish paper in Science, which claimed environmentally relevant concentrations of polystyrene microplastics affected larval fish ecology. That paper was later retracted after investigation and serious misconduct concerns. A retraction does not invalidate the whole microplastics field, but it does show why dramatic claims must be checked for transparent data, appropriate controls, realistic exposure, replication, and conclusions that match the experiment.
The broader lesson was stated clearly by Lenz et al.: microplastic exposure studies should be environmentally realistic. High-dose laboratory effects, artificial particles, and special exposure scenarios may be useful for hazard screening, but they do not prove real-world ecological or human health risk. A credible study must show that the material was plastic, that the dose was realistic, that the particles were representative, and that harm occurred under conditions relevant to actual exposure.
Sources: Wardrop 2016; Sussarellu 2016; Barboza 2018; Lu 2016; Baumann 2016; Mattsson 2015; Lönnstedt & Eklöv 2016/retracted; Berg 2017; Lenz 2016; Gouin 2024
Why are polystyrene bead studies often misleading?
Bottom line: Many harm studies use perfect spherical polystyrene beads at extreme doses.
Those beads are easy to buy and easy to measure, so they are useful for laboratory experiments. They are a poor model for real human exposure. Such beads are not the same chemically as polystyrene we, the public use which is the type present in the environment. For example, that kind of lab make polystyrene is often cross-linked and may contain residues of the cross-linker (divinyl benzene) and surfactants from polymerization. Furthermore, a high-dose study using lab-made polystyrene beads does not show that the irregular, mixed, tiny amounts of plastic found in real life harm people.
This problem was apparent early in the literature: many high-profile harm studies used laboratory polystyrene beads or nanoparticles, while the dominant environmental polymers are usually mixed, weathered PE, PP, PET, fibers, rubber particles, paint particles, and fragments.
Sources: Lenz 2016; Gouin 2024; Wieland 2024; Koelmans 2022, DeArmitt 2020
What is wrong with saying “the science is emerging”?
Bottom line: The measurement methods are still improving, but the main safety question is not new. Plastic particles and common plastic materials have been studied for decades, and the evidence does not show harm at realistic exposure levels.
Calling the science “emerging” can mislead the public. It implies that we are only just beginning to understand whether microplastics are dangerous. That is not true. There are thousands of studies on plastics, polymer toxicology, particle toxicology, dust exposure, food-contact materials, medical polymers, environmental particles, microplastics, and nanoplastics. The evidence base now spans decades.
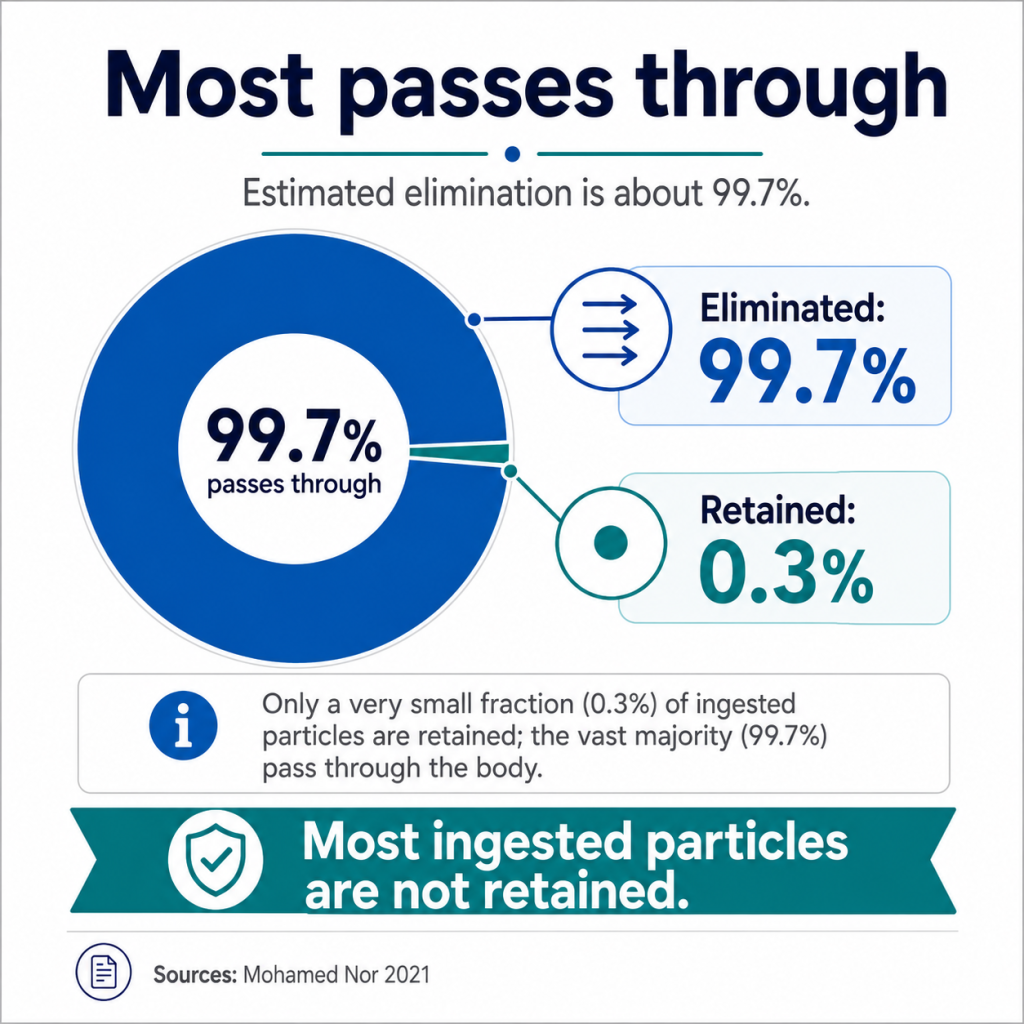
The important question is not whether microplastics can be detected. They can. The important question is whether normal real-world exposure causes harm. On that question, the evidence is already strong: realistic exposure levels are extremely small by mass, most ingested particles pass through the body, retained burden is tiny, and no credible evidence shows human disease caused by normal microplastic exposure.
It is also unlikely that future evidence will overturn this conclusion unless it is exceptionally strong. That is because plastic particles do not have a special physical property that makes them uniquely dangerous. The properties often used to raise concern — small size, hydrophobicity, surface area, persistence, surface charge, biofilm formation, chemical sorption, inhalation, ingestion, and particle transport — are also found in many ordinary dust and environmental particles. These include mineral dust, cellulose fibers, pollen, soot, clay, road dust, pigments, metal particles, glass, ceramics, spores, and organic matter. If those general particle properties do not make the much larger background of ordinary low-toxicity dust uniquely dangerous at normal exposure, they do not automatically make the tiny plastic fraction dangerous either.
This is where Bayesian reasoning matters. Science does not restart with every new headline. Each new claim must be weighed against everything already known. When decades of exposure science, toxicology, materials testing, and particle science show very low risk, a new study must be unusually strong to change the conclusion. It would need to prove confirmed intact plastic particles, realistic exposure, strong contamination control, meaningful retained dose, reproducible harm, and causation rather than mere detection or association.
Most alarming studies do not meet that standard. Many use extreme doses, artificial polystyrene beads, forced exposure routes, weak contamination controls, or particle counts without mass context. Such studies may be useful for method development or hazard screening, but they do not show that everyday exposure harms people.
Therefore, the phrase “the science is emerging” should be used carefully. Analytical methods are developing, and measurements will continue to improve. But the central risk conclusion is not an open blank slate. The current weight of evidence shows no credible reason for public concern about normal real-world exposure to microplastics. Future evidence should still be evaluated, but it should not be allowed to override decades of science unless it is strong enough to prove realistic-dose harm.
Sources: WHO 2022; SAPEA 2019; Koelmans 2022; FDA 2024; Hermsen 2018
Why does decades of evidence matter more than one alarming new study?
Bottom line: Science is cumulative. One alarming study does not reset the evidence to zero.
When scientists say “no credible evidence of harm,” that does not mean nobody has looked. It means the opposite: common plastics have been studied for decades, and realistic human exposure has not been shown to cause disease.
This is the simple idea behind Bayesian updating. Evidence is not judged one headline at a time. Each new claim is weighed against everything already known. If decades of toxicology and exposure evidence show very low risk, then a new study must be exceptionally strong to overturn that conclusion.
A new study should change the conclusion only if it uses realistic doses, proves the particles are plastic, controls contamination, shows harm at real exposure levels, and is independently repeated. Most alarming microplastics studies do not meet those tests. Many use doses far above real life, artificial particles, weak methods, or detection claims that do not prove harm.
The practical conclusion is clear: microplastics are not an untested unknown. New research should continue, but one weak or unrealistic study should not outweigh decades of evidence showing no demonstrated human disease from normal exposure.
Sources: Lenz 2016; Merski 2008; Stock 2021; Koelmans 2022; WHO 2022; FDA 2024; Bradford Hill 1965; Goodman 1999; Ioannidis 2005; Bayes 1763
Do microplastics accumulate in the human body?
Bottom line: Accumulation has not been demonstrated.
Most ingested particles are expected to pass through the digestive tract. Mohamed Nor et al. modeled adult lifetime intake at about 0.015 g and adult tissue burden by age 70 at only about 40.7 ng. That corresponds to a retained mass fraction of roughly 0.00027%, not grams of retained plastic. Claims of large accumulation require direct proof, not assumption. Some studies use the word “accumulation” when they have only detected particles or polymer-associated signals. Accumulation and detection are not the same. Accumulation means increasing retained burden over time, which has not been demonstrated in humans at meaningful levels.
Sources: Nor 2021; Duis 2016; Prata 2022; Inoue 2025; Jovanović 2018; Schwabl 2019; Jovanovic 2018
Can fear of microplastics itself cause harm?
Bottom line: Yes. Excessive fear can cause stress, anxiety, and poor decisions.
Public health communication should reduce risk, not amplify needless fear. People should be told what has been proved, what has not been proved, and how large the exposure actually is.
Sources: Yaribeygi 2017; McEwen 1998; McEwen 2007; Celano 2016; Horenstein 2020
If microplastics are not shown to cause harm, why are people worried?
Bottom line: People are worried because media articles sensationalize and misrepresent the science.
Völker et al. found that scientific articles generally framed microplastic risk as uncertain or unproven, while media coverage overwhelmingly portrayed harm as certain.
Sources: Völker 2020, Yaribeygi 2017; Völker 2020; Covello 1992