Microplastics in the Human Body
Introduction
This section is important because body-location claims attract attention. Answers separate detection, proof of intact plastic, dose, and harm. Laforsch questioned the validity of many studies claiming plastic particles in stool, saliva, sputum, bronchoalveolar lavage fluid, blood, lung tissue, placenta, digestive tract, liver, spleen, and kidney, arguing that many reported particles were consistent with airborne laboratory dust and too large to plausibly enter the claimed tissues through the gut or lungs.
Particle movement in the body is not a new microplastics discovery…
Claims that microplastics or nanoplastics can move through biological barriers are often presented as if they reveal a new and unique plastic hazard. They do not. The movement of small solid particles through the intestinal wall has been discussed since the nineteenth century. Herbst reported finding starch granules in chyle and blood after feeding starch flour to a dog in 1844, and later authors described this phenomenon as “persorption”: the passage of undissolved microparticles through the intestinal wall into lymph or blood. Modern studies and reviews have further examined intestinal particle uptake, Peyer’s patches, M cells, macrophage handling, lymphatic transport, and particle clearance.
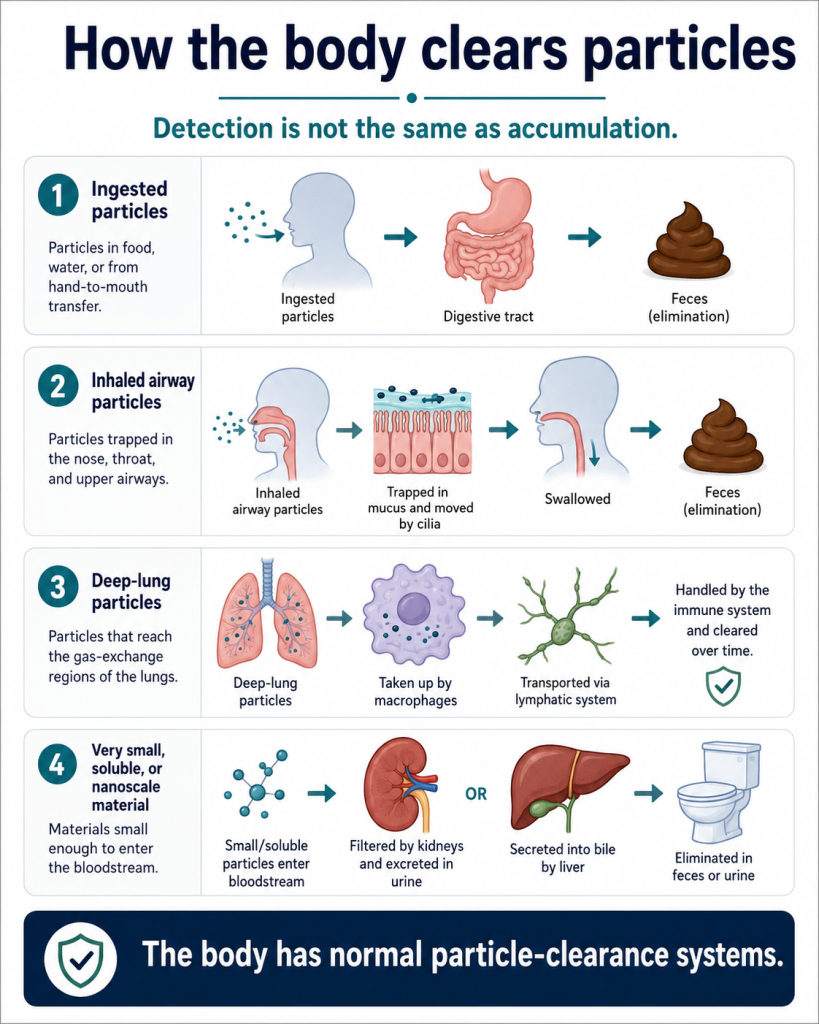
This history is important. It shows that the biological question is not simply whether a particle can move. Very small particles of many types can sometimes cross or be transported across biological barriers under particular conditions. The relevant risk questions are more specific: What is the particle? How large is it? How much is present? Was the material confirmed to be plastic? Was the exposure realistic? Is the particle retained or cleared? Does the retained dose increase over time? Is there reproducible harm at real-world exposure? Detection or possible translocation is therefore not the same as accumulation, toxicity, or disease.
The digestive tract is not an open pathway into the body. It is a selective biological barrier designed to absorb nutrients while excluding most insoluble particles. Older particle-uptake work showed that very small particles can sometimes cross the gastrointestinal barrier under experimental conditions, but that does not mean normal dietary particles accumulate in meaningful amounts. LeFevre and co-workers showed that chronic administration was needed before 5 micrometer particles accumulated in Peyer’s patches in mice, illustrating that uptake is limited and biology-dependent rather than automatic. Powell and co-workers reviewed the origin and fate of dietary nanoparticles and microparticles in the gastrointestinal tract and emphasized that humans are routinely exposed to many non-plastic dietary particles, including mineral particles, without that implying disease. For microplastics, the relevant conclusion is that detection in stool is expected, because most ingested particles are not absorbed and are eliminated. Claims of accumulation therefore require direct evidence of increasing retained mass over time, not merely detection of particles or polymer signals in a sample.
Sources: Herbst 1844; LeFevre 1980; Powell 2010; Mohamed Nor 2021; Schwabl 2019; Zhang 2021; Volkheimer & Schulz 1968; Volkheimer 1974; Geiser 2010; Oberdörster 2004
Have microplastics been found in blood?
Bottom line: Some studies have reported plastic-like particles or polymer signals in blood at extremely low concentrations, but this does not prove harm and detection is uncertain.
Particles in blood are not a new biological concept and are not unique to plastic. Studies published decades ago showed that inhaled or intratracheally instilled ultrafine particles can move from the respiratory tract into blood circulation under experimental conditions. This does not mean that every particle detected in blood is harmful, and it does not prove that normal microplastic exposure causes disease. It means that blood-detection claims must be interpreted in the broader context of ordinary particle exposure, including mineral dust, combustion particles, pigments, soot, metal oxides, biological particles, and other non-plastic material. The key questions remain the same: what was the particle, how much was present, was contamination excluded, was the dose realistic, and was harm demonstrated?
Blood studies are difficult because contamination is easy and the amounts reported are extremely small. A reported signal must be confirmed as real plastic, not lab contamination, background dust, or a method artifact. For perspective, one blood-particle study reported that plastic was only about 1% of detected particles, with pigments and other non-plastic particles making up about 99% (Wu 2023). There is no evidence that the particles cause an effect or that the plastic particles behave differently to the others. The Brits study found chemical signals consistent with plastic polymers in many blood samples, using an improved Py-GC-MS method. But Py-GC-MS destroys the sample, so it does not prove intact plastic particles were present in the blood. It also does not show that the detected material causes harm.
The blood-particle context matters. In one study that analyzed particles in human blood more broadly, plastic accounted for only a small fraction of detected particles, while pigments and other non-plastic particles dominated. That does not prove the non-plastic particles are harmful, but it shows why a plastic-only interpretation is misleading. If the biological question is particle exposure, then all particles should be considered; if the question is plastic-specific risk, then the plastic fraction must be shown to be uniquely toxic or present at a meaningful dose.
Sources: Wu 2023, Brits 2024; Li 2024; Leslie 2022; Rauert 2025; Guan 2023; Nemmar 2002; Shimada 2006; Geiser 2010

Have microplastics been found in the brain?
Bottom line: No reliable study has conclusively proved that intact plastic particles are present in the human brain.
Some studies have reported signals interpreted as plastic, but the main method used can mistake biological material for plastic. This matters especially for the brain because brain tissue is rich in fats and lipids. A chemical signal from a destructive test is not proof of intact plastic particles in the brain.
Particle movement into the brain is not unique to plastic particles. The translocation of inhaled ultrafine particles from the respiratory tract to other organs, including the brain, has been studied for decades. Oberdörster and co-workers reported extrapulmonary translocation of inhaled ultrafine carbon particles in rats and later reported evidence consistent with movement of inhaled ultrafine particles to the olfactory bulb and some brain regions. This does not prove that normal environmental microplastic exposure causes human brain disease. It shows something narrower: very small particles of several kinds can sometimes cross biological barriers under experimental conditions. Therefore, a brain-risk claim must show more than possible particle movement. It must show confirmed plastic identity, realistic exposure, realistic particle type, dose, retained mass, and harm beyond the background of non-plastic particles.
Brain-translocation claims also need particle context. Plastic is not the only particle class studied for movement into, or effects on, the nervous system. Studies have reported brain translocation or neurological associations for several non-plastic particles, including ultrafine carbon, manganese oxide, iron-soot, zinc oxide, titanium dioxide, and black carbon. Some of these particles are more environmentally relevant than laboratory polystyrene nanoparticles because people are actually exposed to combustion particles, mineral particles, metal oxides, and soot. The correct comparison is therefore not “plastic particles versus no particles.” It is plastic particles versus the much larger and better-established background of airborne mineral, combustion, biological, and metal-containing particles.
Sources: Oberdörster 2002; Oberdörster 2004; Oberdörster 2005; Kopatz 2023; Rauert 2025; Mohamed Nor 2021; Chuang 2020; Suglia 2008, Hopkins 2018; Pryor 2022, Liu 2017
Is the claim that the brain contains a large amount of plastic credible?
Bottom line: No. Claims that the brain contains grams of plastic are not credible.
The claim also fails a simple mass-balance check. A person cannot plausibly retain grams of plastic in the brain if estimated lifetime intake is only in the hundredths-of-a-gram range before elimination and modeled retained body burden is at nanogram scale. Any claim of gram-scale plastic accumulation in one organ must explain the source, intake route, retention mechanism, and mass balance. Without that, the number is not merely unproved; it is physically implausible. (Mohamed Nor 2021).
The microscopy images are also limited because the reported particles were described as “putative” microplastics. “Putative” means presumed or suspected, not confirmed. Images or arrows pointing to particles do not establish polymer identity unless the particles are analytically confirmed as plastic and contamination is excluded.
Independent expert reaction to the brain-accumulation claim also raised concerns about interpretation, contamination, analytical uncertainty, and whether the study proved intact plastic particles were present. The Science Media Centre published expert comments from Oliver Jones, Tamara Galloway, Ben Henry, and Antonis Myridakis on the reported accumulation of microplastics in human brain tissue. Those reactions did not establish that the study was false, but they reinforced the key point: the claim requires cautious interpretation because detecting chemical signals or putative particles is not the same as proving intact plastic particles, realistic accumulation, or harm.
Sources: Nihart 2025; Rauert 2025; Monikh 2025; Laforsch 2025; Science Media Centre 2025; Mohamed Nor 2021, Plastics Research Council 2025

Have microplastics been found in lungs?
Bottom line: Lung findings are more plausible than many other tissue claims because people inhale airborne particles.
Even so, finding particles in lung samples does not prove harm. It must be shown that the particles are plastic, that contamination was excluded, and that the dose is enough to cause disease. Plastic dust should also be compared with other inhaled particles such as mineral dust, soot, cellulose, pollen, and fibers.
Sources: Laforsch 2025; Wieland 2022; Jenner 2022; Amato-Lourenco 2021; Vianello 2019
Have microplastics been found in placenta?
Bottom line: Some studies report many types of particles (Bongaerts 2020, Buerki-Thurnherr 2012) including possibly plastic in placenta samples, but they do not prove harm to the fetus.
Placenta studies are highly sensitive to contamination. Detection claims require strong blanks, clean handling, confirmed particle identity, and realistic interpretation. A particle report is not proof of disease or developmental harm. The detection of plastic has been questioned by Laforsch and others. Plastic is one of the many types of particles detected in the body and placenta.
Sources: Laforsch 2025; Bové 2019; Liu 2021; Bongaerts 2020; Buerki-Thurnherr 2012; Clough 2026; Ragusa 2021; Liu 2023; Zhu 2023
Have microplastics been found in stool?
Bottom line: Yes. Stool findings are expected and are not a cause for concern.
Stool detections show that particles including plastics can be swallowed and excreted. That is consistent with elimination rather than accumulation.
Sources: Nor 2021; Mohamed Nor 2021; Schwabl 2019; Zhang 2021
Do detected particles stay in the body or pass through?
Bottom line:
Most ingested particles are expected to pass through; modeled retained amounts are tiny compared with intake
Retention depends on size, shape, surface chemistry, and biology. The evidence shows no accumulation in human, fish or animals. A tiny fraction of very fine particles, including some particles below about 5–10 µm, may cross the gut barrier under certain conditions. Mohamed Nor et al. assumed intestinal absorption of 0.3% of 1–10 µm particles, but that is not the same as retaining 0.3% of total microplastic mass. Using their adult median estimates, modeled tissue burden by age 70 is about 40.7 ng compared with about 0.015 g lifetime intake, meaning more than 99.999% of the modeled lifetime mass is not retained as tissue burden (Nor 2021).
The body also has normal particle-clearance systems. Inhaled particles deposited in the airways and alveoli can be trapped in mucus, cleared by the mucociliary escalator, or engulfed by macrophages. Geiser reviewed macrophage clearance of inhaled micro- and nanoparticles and noted that particles deposited in the airways and alveoli are readily taken up by resident surface macrophages. This process is part of normal lung defense. It does not mean that no particle can ever persist or cause harm, but it does mean that detection of a particle is not the same as accumulation, toxicity, or disease.
Sources: Nor 2021; Duis 2016; Prata 2022; Inoue 2025; Jovanović 2018; Geiser 2010
Have microplastics been found in every human organ?
Bottom line: No. This has not been proved.
Claims of plastic in every human organ are not established. Many reported findings rely on methods that can confuse body fats, lipids, proteins, contamination, or chemical signals with plastic. Some reported particles are also too large to make biological sense in the tissue claimed. The public should not treat these reports as proof that plastic is spread through every organ.
The conclusion is simple: plastic in every organ has not been proved.
Sources: Laforsch 2025; Clough 2026
Have microplastics been found in breast milk, semen, testes, arteries, and other tissues?
Bottom line: Some studies report plastic-associated findings in these samples, but detection is uncertain and does not prove harm.
Each claim must be checked separately. The key questions are whether intact particles were proved, contamination was controlled, dose was realistic, and health effects were actually demonstrated.
Sources: Laforsch 2025; Clough 2026; Ragusa 2022; Zhao 2023; Marfella 2024; Rotchell 2023
Do nanoplastics cross the blood-brain barrier in humans at realistic exposure?
Bottom line: No. This has not been proved.
Nanoparticles of many kinds, not just plastic, can cross the blood-brain barrier under some experimental or medical circumstances. That fact does not prove that environmental nanoplastics cross the human blood-brain barrier at normal exposure levels. Drug-delivery particles are used at high doses and are specially designed to cross biological barriers. Environmental particles are not the same.
One study reported that lab-made polystyrene nanoparticles crossed the blood-brain barrier, but it used an extreme artificial exposure. The particles were not typical environmental plastic, and the dose was about 3,000-9,000 times too high by mass. For the 293 nm particles, the particle count was about 2 trillion times too high. That is not evidence of what happens to people in real life.
Sources: Kopatz 2023; Lenz 2016; Shan 2022; Semmler-Behnke 2008
Do microplastics harm unborn babies, infants, or children at measured exposure levels?
Bottom line: No credible evidence proves that normal measured exposure harms unborn babies, infants, or children.
Some studies report particles or plastic-like signals in placenta, infant stool, or related samples. That does not prove harm. Child and pregnancy claims need especially careful wording because they are emotionally powerful and can easily be overstated.
Sources: WHO 2022; FDA 2024; EFSA 2025; Li 2020; Buerki-Thurnherr 2012
Do microplastics cause inflammation at measured exposure levels?
Bottom line: No credible evidence proves that normal measured exposure causes inflammation.
Some studies report plastic particles causing inflammation, but they lack context. They use exposure levels orders of magnitude higher than realistic environmental exposure. They also fail to mention that any non-toxic particle including dust causes inflammation when the dose is extremely high. As Lenz pointed out, studies are being performed at concentrations a million times (or more) higher than real exposure levels leading to science that can mislead.
Sources: Lenz 2016
Do microplastics harm zebrafish at measured exposure levels?
Bottom line: No credible evidence proves that normal measured exposure causes harm.
Some studies report plastic particles causing effects of plastic particles on zebrafish embryos (Mohan 2023). They use exposure levels order or magnitude higher than realistic environmental exposure. They also fail to mention that any non-toxic particle including dust causes inflammation when the dose is extremely high. Other studies on zebrafish embryos find effects from other particles, dust (Morris, Manjunatha) and even sodium chloride, i.e. table salt (Seli). Such studies are not relevant to human health.
Sources: Lenz 2016; Mohan 2023; Morris 2023; Manjunatha 2021; Seli 2024
Do microplastics persist in the body?
Bottom line: No. Current evidence does not show meaningful long-term accumulation of microplastics in humans at normal real-world exposure levels.
The vast majority of ingested insoluble particles, including plastic particles, are not retained. Mohamed Nor et al. modeled adult lifetime intake at about 0.015 g and adult tissue burden by age 70 at about 40.7 ng, meaning the retained mass fraction is roughly 0.00027%. In particle-count terms, the modeled non-retained fraction is also about 99.8%, but by mass it is greater than 99.999%. Particles that enter tissues may be handled by normal biological defense and clearance systems, including macrophage uptake, lymphatic transport, biliary excretion, renal clearance for sufficiently small or soluble material, and oxidative or enzymatic degradation where the material is susceptible. It has been known for decades that polypropylene degrades rapidly in the body (Liebert 1976) and many other studies show the same (DeArmitt 2017), including for other polymers. This area has been studied extensively in the context of medical plastics implanted in the body (PE hip joints, PP sutures and mesh, PET mesh, PTFE mesh, PMMA eye lenses, various polymers used in pacemakers).
Sources: Liebert 1976; Wagner 2020; DeArmitt 2017